Abstract
Background: Urinary bladder lesions, non-neoplastic and neoplastic, are collectively responsible for significant morbidity and mortality throughout the world. Bladder cancer is a prevalent disease affects a significant number of individuals each year worldwide. The most common non-neoplastic and neoplastic lesion of the urinary bladder is non-specific cystitis and urothelial carcinoma respectively. Objectives: The aim of this study is to describe histopathologic patterns of urinary bladder lesions and associated risk factors in Hawassa University Comprehensive Specialized Hospital from January 2017 to December 2023. Methods: A 7-year cross sectional study was conducted to describe histologically diagnosed bladder lesions and associated factors at Hawassa University Comprehensive Specialized Hospital from January 2017 to December 2023. Results: This study comprised a total of 182 patients who have bladder biopsies at Hawassa University Comprehensive Specialized Hospital, Pathology department from January 2017 to December 2023. Out of which 21 cases (12.1%) are non-neoplastic, while 152 cases (83%) are neoplastic. Nine cases (4.9%) have a descriptive diagnosis. With 139 (90.44%) cases, urothelial neoplasms have the highest frequency form all neoplastic lesions. Ninety-seven cases, or 69.8%, of urothelial neoplasms were invasive; of them, 78 (80.4%) were high grade cases. Low-grade noninvasive papillary carcinomas, which accounted for 24 instances. One case is a cystectomy specimen, and the remaining 181 cases are TURBT. The age range of 50-59 years was the most frequent accounting for 39 (21.4%) of all cases, with a male to female (M: F) ratio of 2.9:1. The most frequent presenting symptom in 146 (85.7%) of patients was hematuria. Conclusions: This study demonstrates that 139 (90.44%) of the neoplastic bladder lesions were bladder neoplasms of urothelial origin, 97 (69.8%) of which are invasive urothelial carcinoma with rising numbers each year and implying the burden in the region.
Keywords
Urothelial Neoplasms, Urinary Bladder Lesions, Cystitis Cystica, Urothelial Papilloma, Invasive Urothelial Carcinoma
1. Introduction
Background
The bladder a hollow muscular organ nestled beneath the peritoneum, functions as storage for urine. Anatomically it joins to the urethra below and the ureters above. The bladder is divided into four structural segments: the fundus, neck, body and apex also known as the dome. The apex reaches towards the abdominal wall and is situated at the anterosuperior aspect. On the other hand, the posteroinferior region is occupied by the fundus also referred to as the base. The large region between the fundus and apex is known as the body. Lastly, the constricted area leading to the urethra is represented by the bladder neck
| [1] | Juan Rosai: Rosai and Ackerman's Surgical Pathology, tenth edition. Philadelphia: Elsevier; 2011. |
| [2] | Shermadou ES, Rahman S, Leslie SW: Anatomy, Abdomen and Pelvis: Bladder. [Updated 2023 Jul 24]. In StatPearls [Internet, Treasure Island (FL): StatPearls Publishing; 2023. |
[1, 2]
.
There are two forms of bladder lesions: on neoplastic and neoplastic. Both types are common and play a major role in the development of clinical signs and symptoms. The non-neoplastic lesions include diseases including Tuberculosis, melakoplakia, urachal lesions and cystitis, all of which have a significant influence on morbidity and contribute to the clinical symptoms. Neoplastic lesions, on the other hand, significantly increase the burden of disease and mortality worldwide
.
Bladder cancer is a disease that is common around the world and claims a large number of lives every year. GLOBOCAN data from 2020 revealed an incidence of 573,000 new BC cases and 213,000 deaths worldwide in 2020 (4). This disease almost 4 times more common in men than in woman, and is closely associated with cigarette smoking. Additionally, the average age of diagnosis for bladder cancer is 71 years old and, the incidence of bladder cancer tends to rise with age
| [4] | GLOBOCAN. 2020, 10: 2020. https://doi.org/10.3322/caac.21660 |
| [5] | Ploeg M, Aben KK, Kiemeney LA: The present and future burden of urinary bladder cancer in the world. World J Urol. 2009, 27: 289-93. https://doi.org/10.1007/s00345-009-0383-3 |
| [6] | Saginala K, Barsouk A, Aluru JS, Rawla P, Padala SA, Barsouk A: Epidemiology of Bladder Cancer. Med Sci (Basel. 2020, 13: 7151633. https://doi.org/10.3390/medsci8010015 |
[4-6]
.
The incidence of BC varies globally with developed communities having greatest rates. However, less developed parts of the world will see a rise in burden of BC. World wide variations in exposure to BC risk factors as well as the age and increase in worldwide population are responsible for these shifts
| [7] | Jozwicki W, Domaniewski J, Skok Z, et al.: Usefulness of histologic homogeneity estimation of muscleinvasive urinary bladder cancer in an individual prognosis: A mapping study. Urology. 2005, 66: 1122-6. https://doi.org/10.1016/j.urology.2005.06.134 |
| [8] | Domanowska E, Jozwicki W, Domaniewski J, et al.: Muscle-invasive urothelial cell carcinoma of the human bladder: Multidirectional differentiation and ability to metastasize. Hum Pathol. 2007, 38: 741-6. https://doi.org/10.1016/j.humpath.2006.11.001 |
| [9] | Lenis AT, Lec PM, Chamie K, Mshs MD: Bladder Cancer: A Review. JAMA. 2020, 17: 1980-1991. https://doi.org/10.1001/jama.2020.17598 |
[7-9]
. Bladder cancer is a disease with many different forms, the most common of which is urothelial cancer, highlighting its importance in the disease spectrum. More than 90% of cases are bladder cancers, most of which are urothelial malignancies. Typically, urothelial cancer is observed in its pure form. However, it is noteworthy that divergent differentiation or aberrant histologic characteristic can be present in BC. Studies that particularly focus on studying these patterns have found that the prevalence of these differentiation patterns in urothelial carcinoma varies, with estimates ranging from 7% to 81
| [7] | Jozwicki W, Domaniewski J, Skok Z, et al.: Usefulness of histologic homogeneity estimation of muscleinvasive urinary bladder cancer in an individual prognosis: A mapping study. Urology. 2005, 66: 1122-6. https://doi.org/10.1016/j.urology.2005.06.134 |
| [8] | Domanowska E, Jozwicki W, Domaniewski J, et al.: Muscle-invasive urothelial cell carcinoma of the human bladder: Multidirectional differentiation and ability to metastasize. Hum Pathol. 2007, 38: 741-6. https://doi.org/10.1016/j.humpath.2006.11.001 |
| [10] | Mazzucchelli R, Marzioni D, Tossetta G, Pepi L, Montironi R: Bladder Cancer Sample Handling and Reporting: Pathologist's Point of View. Front Surg. 202128, 754741: https://doi.org/10.10.3389/fsurg.2021.754741 |
[7, 8, 10]
. The most common clinical presentation of bladder cancer is gross hematuria, but patients can also present with isolated microscopic hematuria (urinalysis showing 3 red blood cells per high-power field), lower urinary tract irritative symptoms, or a mass that incidentally discovered on imaging. So, to have an accurate and definitive diagnosis histopathology is the only resort
| [11] | Bayraktar Z, Gurbuz G, Taşci AI, Sevin G: Staging error in the bladder tumor: the correlation between stage of TUR and cystectomy. Int Urol Nephrol. 2001: 627-9. https://doi.org/10.1023/a: 1020553812554 |
| [12] | Chalasani V, Chin JL, Izawa JI: Histologic variants of urothelial bladder cancer and nonurothelial histology in bladder cancer. Can Urol Assoc J. 2009, 4: 193-8. https://doi.org/10.5489/cuaj.1195 |
| [13] | Cumberbatch MGK, Jubber I, Black PC, et al.: Epidemiology of bladder cancer: a systematic review and contemporary update of risk factors in 2018. Eur Urol. 2018, 74: 784-795. https://doi.org/10.1016/j.eururo.2023.03.029 |
[11-13].
Bladder biopsies can be obtained from transurethral resection (TUR) or cystectomy specimens. Standard radical cystectomy specimens encompass the distal sections of the ureters, prostate, and seminal vesicles in men, or the urethra, adjacent vagina, and uterus in women. These adjacent organs and the peritoneal lining aid in orienting the surgical specimen during analysis. In contrast, TUR specimens are collected through a cystoscope using tools like cold cup forceps, diathermy forceps, or a small diathermy loop. The fragments obtained are then sent to pathology, assisting in pathologic staging and contributing valuable information for the diagnosis and management of urinary bladder lesions
| [14] | Wu X, Ros MM, Gu J, Kiemeney L (2008: Epidemiology and genetic susceptibility to bladder cancer. BJU Int. 102: 1207-1215. https://doi.org/10.1111/j.1464-410X.2008.07961.x |
| [15] | Global cancer observatory. International Agency for Research on Cancer, WHO. Incidence, Mortality, 2020. |
| [16] | Adeloye D, Harhay et. al: Estimate of the incidence of bladder cancer in Africa: A systematic review and Bayesian meta-analysis. Int J Urol. 2019, 26: 102-112. https://doi.org/10.1111/iju.13824 |
[14-16]
.
Due to rising awareness and the development of more precise and sensitive indicators, urothelial carcinoma has come under more scrutiny in recent years. This increased focus has highlighted the often-observed heterogeneous differentiations in urothelial carcinoma. The most common variations are micropapillary, sarcomatoid, glandular, and squamous. Remarkably, non-urothelial histologies such squamous, adenocarcinoma, and small cell carcinoma are frequently observed in advanced stages of bladder cancer. Further prospective investigations are necessary to better understand the prognosis of patients with these variations and to develop customized therapeutic methods. Future research must continue to focus on gaining more precise insights into the prognosis and best treatment approaches for these varied appearances
.
2. Materials and Methods
2.1. Study Area
The research was conducted at the pathology department of the Hawassa University Comprehensive Specialized Hospital (HUCSH), situated in Hawassa, a city located approximately 275 kilometers south of Addis Ababa, Ethiopia's capital. Hawassa is home to around 280,000 residents and enjoys a moderate climate. The city’s healthcare infrastructure includes four primary hospitals managed privately and two operated by the government. Additionally, the city has numerous public and private clinics and pharmacies. A government university, which serves as an educational center for the region, is also located in Hawassa. Established in 2005, the Hawassa University College of Medicine and Health Sciences uses HUCSH as its primary referral hospital, and it functions as a key teaching facility for the college. Within HUCSH, the pathology department plays a critical role, specializing in the analysis of blood, biopsy, and cytology specimens obtained from various healthcare facilities in the region, both public and private. The department is staffed by nine pathologists, eleven pathology residents, and seven histotechnicians, making it a central component of diagnostic and teaching services in the institution.
2.2. Study Design and Period
This study employed a cross-sectional design, focusing on data retrieved from the archives of the pathology department. The data comprised patient records registered between January 2017 and December 2023. This approach allowed the study to analyze a wide range of cases within this six-year period, offering a comprehensive view of trends and patterns in bladder pathology.
2.3. Population
2.3.1. Source Population
The source population included all patients who had biopsy specimens submitted to the pathology department from January 2017 to December 2023. This broad population base ensured that a diverse range of cases was captured, allowing for a detailed analysis of pathology trends.
2.3.2. Study Population
The study population was further refined to include only those patients whose bladder biopsy specimens were submitted to the pathology department within the same time frame. This specific focus on bladder biopsies enabled the research to provide more targeted insights into bladder-related pathologies.
2.3.3. Inclusion Criteria
The study included original hard copy reports of bladder lesions, provided these reports contained all the necessary information, along with patient medical charts from January 2017 to December 2023. This criterion ensured that the data used for analysis was complete and accurate, contributing to the study’s reliability.
2.3.4. Exclusion Criteria
Reports that lacked a histologic diagnosis were excluded from the study. This exclusion helped maintain the integrity of the data, ensuring that only cases with full diagnostic information were analyzed.
Sample Size and Sampling Technique / Sampling Procedures
All patients who met the inclusion criteria during the study period were included in the analysis. The sample size was calculated using the single population proportion formula, expressed as n = Z² * p(1 - p) / d². In this formula, "Z" represents the confidence level at 95% (with a standard value of 1.96), "d" is the margin of error set at 5%, and "p" is the estimated prevalence of neoplastic bladder lesions based on previous studies, which was 68.1%. By substituting these values into the formula, the calculated sample size was 334. Given that the source population comprised 350 individuals, the final sample size was adjusted using the finite population correction formula, resulting in a final sample size of 172 patients. This rigorous calculation ensured that the sample was representative of the larger population, allowing for reliable statistical analysis.
2.3.5. Study Variables
The study examined a range of variables, categorized as independent and dependent.
Independent variables included
1. The patient’s age at diagnosis (in years)
2. Sex,
3. Clinical presentation
4. Size of the biopsy sample (in centimeters),
5. Duration of the lesion (in months), and
6. The presence or absence of muscle proper in transurethral resection of bladder tumor (TURBT) specimens.
The dependent variable was
The occurrence of neoplastic bladder lesions. By analyzing these variables, the study sought to identify potential risk factors and patterns associated with bladder pathologies.
2.4. Data Collection Tools and Procedures
Data collection was conducted using a systematic approach to ensure accuracy and consistency. Hard copies of all cases with histopathological diagnoses of bladder lesions were retrieved using biopsy code numbers. Trained data collectors then extracted the relevant information, including demographic data, clinical presentation, type of bladder specimen, and histopathological diagnosis, using a structured data extraction checklist. This methodical approach ensured that all necessary data was collected in a uniform manner, minimizing the risk of errors and ensuring the integrity of the research.
2.5. Operational Definitions
Several key operational definitions were established to guide the study. A urothelial lesion was defined as any abnormal change in the integrity and intensity of bladder tissue. Histopathologic pattern referred to the observable arrangement and characteristics of cells and tissues under a microscope on a biopsy specimen, providing critical insights into the specific diagnosis. These definitions were essential for maintaining clarity and consistency throughout the research process.
2.6. Data Analysis Procedures
The data collected were analyzed using the Statistical Package for Social Sciences (SPSS) version 20. Descriptive analyses were conducted to summarize the frequency and distribution of bladder lesions within the study population. Additionally, binary logistic regression was used to explore the relationships between the study participants and the selected variables. This statistical analysis allowed the study to identify potential correlations and trends, providing deeper insights into the factors influencing the occurrence of neoplastic bladder lesions.
2.7. Data Quality Management
To ensure the reliability of the study findings, stringent data quality management procedures were implemented. These included regular checks for accuracy during data collection and entry, as well as continuous monitoring to identify and resolve any discrepancies. By adhering to these rigorous quality control measures, the study ensured that its conclusions were based on accurate and reliable data. The data was be checked for completeness, cleaned, and coded for entry and analysis by the principal investigator.
2.8. Ethical Consideration
Ethical clearance and approval was obtained from the institutional review board (IRB) of Hawassa University College of medicine and health science. A formal letter is obtained from HUCSH's chief clinical director and Department of Pathology to get patients' medical record charts and collect report formats. The confidentiality of study the patient’s data was kept a secret.
2.9. Dissemination Plan
Results of this study were presented to the department of pathology, public health & school of medicine staff, and other interested bodies. Copy of the final research was given to HUCSH. Every effort was made to publish the research findings in peer-reviewed reputable national and international journals. Write it in descriptive form.
3. Results
This study included 182 cases that met the study criteria. Neoplastic bladder lesions present in 152 (83.5%) of cases with urothelial neoplasms account for 139 (90.44%) cases. Ninety-seven cases, or 69.8%, of urothelial neoplasms were invasive; of them, 78 (80.4%) were high grade cases. Low-grade noninvasive papillary carcinomas, which accounted for 24 instances. The age range of 50-59 years was the most frequent for cases, with a male to female (M: F) ratio of 2.9:1. The most frequent presenting symptom in 85.7% of patients was hematuria. There has been a steady rise in the number of biopsies submitted to the pathology department of HUCSH with highest number recorded in 2023 with 41 (22.5%) and there was a significant association with age and sample size received with the neoplastic nature of the lesion. (
Table 1)
Neoplastic bladder lesions were present in 152 (83.5%) of the total patients. Urothelial neoplasms account for 139 (91.44%) cases. They were followed in frequency by 6 (3.94%), squamous cell carcinoma, 2 (1.32%), poorly differentiated carcinoma, 1 (0.65%), myxoid leiomyosarcoma, 1 (0.65%), secondary carcinoma from the prostate, 1 squamous papilloma (0.65%) and 1 primary mucinous adenocarcinoma. (
Table 1)
The majority of cases of urothelial neoplasms were invasive, accounting for 97 cases or 69.8%. These were followed by non-invasive urothelial neoplasms which account for 30.2% of them among them low-grade noninvasive papillary carcinomas accounted for 24 cases (17.2%), high-grade noninvasive papillary carcinomas, which accounted for 13 cases (9.4%), PUNLMP 3 cases (2.2%), and 2 (1.4%) cases of urothelial papilloma. (
Table 1).
Among the 97 invasive urothelial carcinomas, 19 (19.6%) of them are low grade and 78 (80.4%) are high grade. 15 (15.5%) cases of invasive high-grade papillary urothelial carcinomas show squamous differentiation; 1 (1%) case is nested urothelial carcinoma, and 1 (1%) is microcystic urothelial carcinoma. Out of 97 invasive urothelial carcinomas 49 (50.5%) are invading the lamina propria and 48 (49.5%) are muscle invasive.
Of the 152 neoplastic bladder tumors, 43 (28.3%) are pTa, 53 (34.8%) are pT1, 51 (33.55%) are pT2, 1 (0.65%) is pT3, and 2 (1.3%) are pT4a with metastasis to the prostate, and 2 (1.3%) cases were not staged.
Table 1. Frequency of neoplastic and non-neoplastic bladder lesions in HUCSH from January 2017-December 2023.
Type of the lesion | Frequency | Percent |
Non neoplastic lesions |
Chronic nonspecific cystitis | 7 | 33.33% |
Cystitis cystica | 7 | 33.33% |
TB cystitis | 3 | 14.28% |
Schistosomiasis | 1 | 4.76% |
Interstitial cystitis | 1 | 4.76% |
Polypoid cystitis | 1 | 4.76% |
Eosinophilic cystitis | 1 | 4.76% |
Total | 21 | 100% |
Neoplastic bladder lesions |
Urothelial neoplasms | 139 | 91.44% |
Squamous cell carcinoma | 6 | 3.94% |
Poorly differentiated carcinoma | 2 | 1.32% |
Myxoid leiomyosarcoma | 1 | 0.66% |
Secondary carcinoma | 1 | 0.66% |
Primary mucinous adenocarcinoma | 1 | 0.66% |
Collision tumor invasive urothelial with squamous cell carcinoma | 1 | 0.66% |
Squamous papilloma | 1 | 0.66% |
Total | 152 | 100% |
Urothelial neoplasms |
Invasive | Invasive urothelial carcinoma | 97 | 69.8% |
Noninvasive | Noninvasive LGPUC | 24 | 17.2% |
Noninvasive HGPUC | 13 | 9.4% |
PUNLMP | 3 | 2.2% |
Urothelial papilloma | 2 | 1.4% |
Total | 139 | 100% |
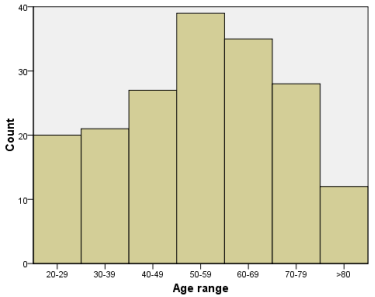
Figure 1. Distribution of age in decades of patients with bladder lesions in |HUCSH from January 2017- December 2023.
The patients in this study were aged from 20 to 95 years, with the mean age of 53.45 years (SD=17.524). The largest group of patients is 50- 59 years old (
figure 1).
Of all the 182 patients, 135 (74.2%) were men and 47 (25.6%) were female; the male to female ratio (M: F) was 2.9:1.
Of neoplastic lesions these, the male to female ratio was 3.13:1, with 115 (75.84%) being male and 36 (24.16) being female. The sixth and seventh decades were the peak age of presentation.
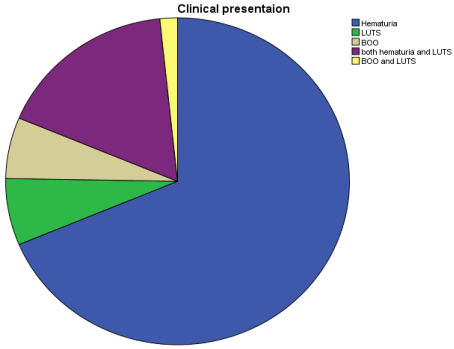
Hematuria was the most common clinical manifestation, occurring in 85.7% of patients, and is followed by LUTS. (
Figure 2) Its mean duration is ten months, and ranges from two weeks to ten years. 164 cases (93.4%) of bladder cancer have been clinically diagnosed; genitourinary TB accounts for seven cases (3.8%), prostatic carcinoma with bladder wall invasion for four cases (2.2%), interstitial cystitis for one case (0.5%), and six cases have no clinical diagnosis written.
Figure 2. Distribution of clinical features of all cases in HUCSH from January 2017 to December 2023.
Out of 182 biopsies evaluated only 1 case is a cystectomy specimen with a diagnosis of primary mucinous adenocarcinoma the rest 181 cases are TRUBT. Out of 181 TURBT specimens with the average sample size of 3.9 cm, the size ranges from 0.3-18 cm.
Neoplastic tumors were found in 151 cases out of 181 TURBT specimens. Muscle proper was not represented in 34 cases (23%), but it was represented in 88 cases (58%). It was not stated in the pathology result in 29 cases (19%) whether or not muscle proper was represented.
Of 88 cases of TURBT specimens in which muscle proper was represented, 53 case shows muscle invasion making the stage pT2 of 53 case of muscle invasive urothelial carcinoma seen in TURBT specimens, 52 cases were high grade invasive papillary urothelial carcinoma and 1 case was low grade invasive papillary urothelial carcinoma.
There are 16 (11.67%) recurrent tumors out of 152 neoplastic tumors among those tumors 13 (81.25%) were invasive urothelial carcinomas, 2 (12.5%) are low grade noninvasive papillary urothelial carcinomas and 1 (6.25%) case was non diagnostic. The recurrent tumors have a previous diagnosis of invasive urothelial carcinoma (pT1) in 7 (43.75%), LGPUC in 5 (31.25%), HGPUC in 2 (12.5%) and in 2 recurrent tumors the previous diagnosis could not be obtained. The time of recurrence spans from 1 year to 6 years with mean of 2 year and 2 months and the most common time to have a recurrence being 1 year in 31.25% of the recurrent tumors.
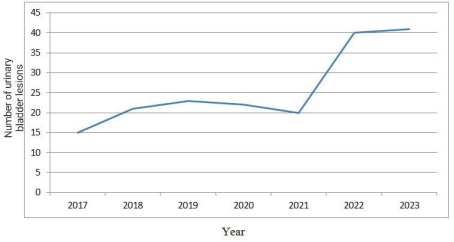
There has been a steady rise in the number of biopsies submitted to the pathology department of HUCSH with highest number recorded in 2023 with 41 (22.5%) cases followed by 40 (22%) in 2022, 23 (12.5) in 2019,22 (12.1) in 2020, 21 (11.5) in 2018, 20 (11%) in 2021 and 15 (8.2%) in 2017. (
Figure 3) The non-neoplastic lesions are, evenly distributed throughout the study period where as there has been an increase in neoplastic bladder lesions majority being invasive urothelial carcinoma. (
Table 2)
Table 2. Trends of urothelial carcinoma in HUCSH from January 2017 to December 2023.
Urothelial neoplasms | Year of biopsy report | Total |
2017 | 2018 | 2019 | 2020 | 2021 | 2022 | 2023 |
Invasive Urothelial carcinoma | 3 | 6 | 7 | 8 | 14 | 28 | 31 | 97 |
Noninvasive LGPUC | 4 | 6 | 5 | 3 | 2 | 0 | 4 | 24 |
Noninvasive HGPUC | 2 | 4 | 5 | 2 | 0 | 0 | 0 | 13 |
PUNLMP | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 3 |
Urothelial papilloma | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 2 |
Total | 9 | 17 | 19 | 12 | 17 | 29 | 35 | 139 |
Figure 3. Trends of urinary bladder lesions in HUCSH from January 2017 to December 2023.
Factors Associated with Neoplastic Bladder Lesions
Bivariate analysis was done to identify factors associated with neoplastic and non-neoplastic bladder lesions. Based on analysis age, sex, duration of the lesion and received sample size were significantly associated with neoplastic lesions.
For factors which showed significant association in bivariate analysis, multivariate logistic regression analysis was done. In multivariate logistic regression, age of 40-59 years (AOR=5.918; 95% CI: 1.903-18.404) and >60 years (AOR=8.928; 95% CI: 2.729-29.203), sample size received 3.1-6cm (AOR=6.053; 95% CI: 1.756-20.862) and >6cm (AOR=6.053; 95% CI: 1.075-82.712), showed significant association with the neoplastic lesions.
Table 3. Factors associated with the neoplastic bladder lesions in HUCSH from January 2017 to December 2023.
Variables | Categories | Biologic nature | COR (95% CI) | AOR (95%CI) |
Neoplastic N (%) | Non neoplastic N (%) |
Age | 20-39 | 25(70) | 16(30) | R | R |
40-59 | 8(12.1) | 58(87.9) | 4.64(1.76-12.235) * | 5.918 (1.903-18.404)** |
> 60 | 6(8) | 69(92) | 7.36(2.592-20.904) * | 8.928 (2.729-29.203)** |
Sex | Male | 116(85.9) | 19(14.1) | 1.865(0.812- 4.284) * | 1.430 (0.543-3.771) |
Female | 36(76.6) | 11(13.4) | R | R |
Duration of the lesion | 0-6month | 81(78.6) | 22(21.4) | R | R |
7-12month | 39(86.7) | 6(13.3) | 1.765(0.662-4.705) | 2.429 (0.786-7.509) |
>12month | 28(96.5) | 1(3.5) | 7.605(0.979-59.048) * | 6.629 (0.791-55.583) |
Received sample size | 0-3cm | 69(73.4) | 25(26.6) | R | R |
3.1-6cm | 55(93.2) | 4(6.8) | 4.982(1.636-15.167)* | 6.053 (1.756-20.862)** |
>6cm | 28(96.5) | 1(3.5) | 10.145(1.311-78.526)* | 9.428 (1.075-82.712)** |
4. Discussion
Bladder cancer is the seventh most frequent type of cancer worldwide. Globally, bladder cancer takes a significant impact on lives each year. This study comprised a total of 182 patients the majority 151 cases (83%) are neoplastic. With 139 (90.44%) cases, urothelial neoplasms were the most common form of neoplastic lesions. The age range of 50-59 years was the most common for cases, with a male to female (M: F) ratio of 2.9:1. There has been a steady rise in the number of biopsies submitted to the pathology department of HUCSH and a significant association with age and sample size received with the neoplastic nature of the lesion.
Eighty-three percent of bladder lesions were neoplastic lesions, which was similar to the seventy-nine percent study conducted in India
. In our analysis of non-neoplastic bladder lesions, cystitis cystica and chronic nonspecific cystitis accounted for 33.33% each of all non-neoplastic bladder lesions. This was in comparison to a study conducted in Patan, Nepal, where chronic nonspecific cystitis accounted for 21.4% of non-neoplastic lesions, followed by cystitis cystica
and tuberculous cystitis for 14.28% of non-neoplastic cases
.
Among the neoplastic bladder lesions there were 2 Urothelial papillomas which is the most common benign neoplastic lesion in this study accounting for which is comparable to the study done on Nigeria which there was only 4 urothelial papillomas
| [21] | Sasikumar, S., Wijayarathna, K. S. N. et. al: A., & Abeygunasekera, A. M. Pathological Characteristics of Primary Bladder Carcinoma Treated at a Tertiary Care Hospital and Changing Demographics of Bladder Cancer in Sri Lanka. Advances in Urology. 201616, https://doi.org/10.1155/2016/5751647 |
[21]
. and a single case of squamous papilloma.
Urothelial carcinomas make up 91.95% of bladder cancer cases, which is comparable to research conducted at Lister Hospital in Stevenage, Hertfordshire, UK, which reported that 92% of bladder cancer cases had urothelial carcinoma
| [22] | C. Aparna, M. D, Rayapa Reddy Thumma, C Padmavathi Devi, S V R L Jyothi Vanapalli, T D N Mounika: histological Spectrum of Urothelial Lesions - Experience of A Single Tertiary. Care Institute, international Journal of Contemporary Medical Research Volume 3 | Issue 6 | June. 2016. |
[22]
. According to a study conducted in Ethiopia, the most frequent malignant bladder tumor (80.4%) is urothelial carcinoma
| [23] | Anita Shah, Manglesh Srivastava, Ashok Samdurkar, Ghanshyam Sigdel SPECTRUM OF LESIONS IN URINARY BLADDER: A HISTOPATHOLOGICAL STUDY Journal of Universal College of Medical Sciences. 6: 24-27. https://doi.org/10.3126/jucms.v6i2.22473 |
[23]
.
Invasive urothelial carcinomas accounted for 69.8% of all urothelial neoplasms in this study, making it the most common type. This is similar to a study conducted at Subharti Medical College in Meerut, India
| [19] | Manisha Shrestha1, Dipti Gautam1, Prakriti Shah1, Prateek Krishna Shrestha: Histopathological Spectrum of Nonneoplastic and Neoplastic Lesions of Urinary Bladder Nepalese Medical Journal, (2021) Vol. 4, 473- 477. https://doi.org/10.7860/NJLM/2021/46894.2537 |
[19]
where invasive urothelial carcinomas accounted for 60.8% of all urothelial neoplasms. Of all invasive urothelial carcinomas in this study, 19.5% are low grade and 80.4% are high grade, which is comparable to a study conducted in India that found high grade urothelial carcinomas to be the most common type of invasive urothelial carcinomas, accounting for 51.4% of all invasive neoplasms. 15.5% of invasive urothelial carcinomas displayed squamous differentiation, which is higher than the 6% variant histologic differentiation found in an Egyptian study
| [24] | A CLINICO-HISTOPATHOLOGICAL STUDY OF URINARY BLADDER LESIONS Siddhi Kumari Pandey1, Ranu Tiwari Mishra2, F: S. Solanki3, Sanjay Totade4, Jagmohan Singh Dhakar5International Journal of Academic Medicine and Pharmacy. ISSN (O):: 2687-5365. |
[24]
and lower than a study conducted in the USA that found 19.5% variant histologic differentiation
| [25] | El-Siddig AA, Albasri AM, Hussainy AS, Alhujaily AS: Urinary bladder cancer in adults: a histopathological experience from Madinah, Saudi Arabia. J Pak Med Assoc. 2017, 67: 83-86. |
[25]
Non-invasive urothelial carcinomas accounted for 30.2% of cases, following invasive urothelial carcinomas. This percentage is comparable to a study conducted in Nigeria, where non-invasive urothelial carcinomas accounted for 29.7% of cases. After invasive urothelial carcinoma, noninvasive low-grade and noninvasive high grade urothelial carcinomas were observed in 17.2% and 9.4% of urothelial neoplasms, respectively, low grade was the most prevalent type of non-invasive urothelial carcinoma, which was consistent with a study conducted in Ethiopia where low grade was also common
| [23] | Anita Shah, Manglesh Srivastava, Ashok Samdurkar, Ghanshyam Sigdel SPECTRUM OF LESIONS IN URINARY BLADDER: A HISTOPATHOLOGICAL STUDY Journal of Universal College of Medical Sciences. 6: 24-27. https://doi.org/10.3126/jucms.v6i2.22473 |
[23]
. and 2.2% of PUNLMP, which was similar to a study conducted in India where 5.6% of participants had PUNLMP
| [21] | Sasikumar, S., Wijayarathna, K. S. N. et. al: A., & Abeygunasekera, A. M. Pathological Characteristics of Primary Bladder Carcinoma Treated at a Tertiary Care Hospital and Changing Demographics of Bladder Cancer in Sri Lanka. Advances in Urology. 201616, https://doi.org/10.1155/2016/5751647 |
| [26] | Forae, GeraldDafe & Ugiagbe, EzekielEnoghama & Mekoma, DikeFidelis. (2016: A descriptive study of bladder tumors in Benin City, Nigeria: An analysis of histopathological patterns. Saudi surgical journal. 4: 113. https://doi.org/10.4103/2320-3846.193986 |
[21, 26]
. of all 182 bladder lesions 9 (4.9%) have a descriptive diagnosis which is similar to a study done in Jinnah medical center, Karachi, Pakistan 3.1% of bladder biopsies have a descriptive diagnosis
| [27] | Muhammed Mubarak, Javed I. Kazi, Altaf Hashmi, Manzoor Hussain, Syed Anwer Naqvi, Syed Adeebul Hassan Rizvi: Urinary Bladder Tumors in Southern. Pakistan: A Histopathological Perspective, Middle East Journal of Cancer; July. 2014, 5: 167-173. |
[27]
.
In addition to the urothelial carcinomas, squamous cell carcinomas account for 4% of malignant bladder neoplasms which was lower than a study done in Egypt 13.8%
. but similar to the study done in Addis Abeba, Ethiopia where squamous cell carcinoma account for 5.2% of the cases
| [23] | Anita Shah, Manglesh Srivastava, Ashok Samdurkar, Ghanshyam Sigdel SPECTRUM OF LESIONS IN URINARY BLADDER: A HISTOPATHOLOGICAL STUDY Journal of Universal College of Medical Sciences. 6: 24-27. https://doi.org/10.3126/jucms.v6i2.22473 |
[23]
. Among 151 neoplastic TURB specimens muscle proper was not represented in 34 cases (23%), but it was represented in 88 cases (58%). It was not stated in the pathology result in 29 cases (19%) whether or not muscle proper was represented, which is comparable to the study done in USA where muscle represented in 52.1 % absent in 30.2% and not mentioned in 17.7%
.
A total of 182 bladder biopsy specimens were assessed in this study; of these, 99.4% were TURBT specimens. This percentage was comparable to that of a study conducted in Brazil, where 165 specimens (100%) were TURBT
| [30] | Billis A, Schenka AA, Ramos CC, Carneiro LT, Araújo V: Squamous and/or glandular differentiation in urothelial carcinoma: prevalence and significance in transurethral resections of the bladder. Int Urol Nephrol. 2001: 631-3. https://doi.org/10.1023/a: 1020597611645 |
[30]
. 1 (0.6%) cystectomy specimen which is lower than a study done in Jabalpur, India 16% were cystectomy samples
| [31] | Wasco MJ, Daignault S, Zhang Y, Kunju LP et. al: Urothelial carcinoma with divergent histologic differentiation (mixed histologic features) predicts the presence of locally advanced bladder cancer when detected at transurethral resection. Urology. 2007, 70: 69-74. https://doi.org/10.1016/j.urology.2007.03.033 |
[31]
. The average age of patients with bladder lesions was 53.42 years. This outcome agreed with research conducted in Nigeria (54.9 years)
| [32] | Shah RB, Montgomery JS, Montie JE, Kunju LP: Variant (divergent) histologic differentiation in urothelial carcinoma is under-recognized in community practice: impact of mandatory central pathology review at a large referral hospital. Urol Oncol. 2013, 31: 1650-5. https://doi.org/10.1016/j.urolonc.2012.04.009 |
[32]
. Bladder lesions were more common in men than in women. Specifically, the ratio of male to female (M: F) was 2.9:1, which was consistent with the results of a study conducted in India (M: F 3.1:1)
| [33] | Boustead GB, Fowler S, Swamy R, Kocklebergh R, Hounsome L: Section of Oncology, BAUS. Stage, grade and pathological characteristics of bladder cancer in the UK: British Association of Urological Surgeons (BAUS) urological tumour registry. BJU Int. 2014, 113: 924-30. https://doi.org/10.1111/bju.12468 |
[33]
. Neoplastic bladder lesions have a male to female ratio of 3.13:1. This ratio was comparable to that of a study conducted in Sri Lanka's Colombo South Teaching Hospital, which found a male to female ratio of 4.1:1
.
Hematuria is the most prevalent clinical manifestation in this study, occurring in 85.7% of cases; this is comparable to a study conducted in Ethiopia (91.8%)
| [23] | Anita Shah, Manglesh Srivastava, Ashok Samdurkar, Ghanshyam Sigdel SPECTRUM OF LESIONS IN URINARY BLADDER: A HISTOPATHOLOGICAL STUDY Journal of Universal College of Medical Sciences. 6: 24-27. https://doi.org/10.3126/jucms.v6i2.22473 |
[23]
.
There are 11.67% recurrent tumors out of 137 urothelial cancers among those tumors 13 (81.25%) were invasive urothelial carcinomas, 2 (12.5%) are low grade noninvasive papillary urothelial carcinomas and 1 (6.25%) case was non diagnostic. The most common previous diagnosis being invasive urothelial carcinoma in 43.75%. The time of recurrence spans from 1 year to 6 years with mean of 2 year and 2 months and the most common time to have a recurrence being 1 year in 31.25% of the recurrent tumors which is lower than a study done in Addis Ababa, Ethiopia where there was a 31% recurrence with mean time of recurrence of 8 months, another study done in McGill University Health Centre, Montréal the overall rate of recurrence for NMIBC is 60% to 70%, and the overall rate of progression is 20% to 30%
| [35] | Chamie K, Ballon-Landa E, Bassett JC, Daskivich TJ, Leventhal M, Deapen D, Litwin MS: Quality of diagnostic staging in patients with bladder cancer: a process-outcomes link. Cancer. 2015, 1: 379-85 https://doi.org/10.1002/cncr.29071 |
[35]
. In other study done in Shanghai, China, patients with bladder tumor completely removed with TURBT, up to 50% of these was a recurrence of cancer within 12 months
| [36] | Hodges KB, Lopez-Beltran A, Maclennan GT, Montironi R, Cheng L: Urothelial lesions with inverted growth patterns: histogenesis, molecular genetic findings, differential diagnosis and clinical management. BJU Int. 2011, 107: 532-7. https://doi.org/10.1111/j.1464-410X.2010.09853.x |
[36]
.
Cases whose age is between 40-59 year and >60 year are 5.9 times and 8.9 times more likely to be neoplastic than younger age group (20-39 year) respectively. Which align with a Globocan data that shows a total of 90% of bladder cancer diagnoses are made in those 55 years of age and older
. Aged ≥65 years have 11 times higher incidence than those younger than 65 years
| [37] | Dive AM, Bodhade AS, Mishra MS, Upadhyaya N: Histological patterns of head and neck tumors: An insight to tumor histology. J Oral Maxillofac Pathol. 2014, 18: 58-68. https://doi.org/10.4103/0973-029X.131912 |
[37]
. Also agree with the study done in Romania where the highest incidence of bladder tumors was recorded in the individuals aged between 60 and 79 years old
| [38] | Cao M, Yang G, Pan et. al: Repeated transurethral resection for non-muscle invasive bladder cancer. Int J Clin Exp Med. 2015, 15: 1416-9. |
[38]
.
Bladder lesions whose size are between 3.1 and 6 cm and >6cm are 4.92 times and 10.145x more likely to be neoplastic than specimens that are less than 3 cm respectively indicating the importance of having large sample size in diagnosis of neoplastic bladder lesions however, no study was found that associated gross sample size received and biologic nature of the bladder lesion. Association was not found between sex, clinical symptoms and duration of the lesion and the biologic nature of the lesion. Global cancer analyses have shown that male-gender is four times more likely to develop bladder cancer than female gender
| [38] | Cao M, Yang G, Pan et. al: Repeated transurethral resection for non-muscle invasive bladder cancer. Int J Clin Exp Med. 2015, 15: 1416-9. |
| [39] | Hamdi Y, Abdeljaoued-Tej I, Zatchi AA, Abdelhak S, Boubaker S, Brown JS, Benkahla A: Cancer in Africa: The Untold Story. Front Oncol. 2021, 15: 650117. https://doi.org/10.3389/fonc.2021.650117 |
| [40] | Dora, Jakus., Ivan, Šolić., J. et. al: The Impact of the Initial Clinical Presentation of Bladder Cancer on Histopathological and Morphological Tumor Characteristics. 12: 4259-4259. https://doi.org/10.3390/jcm12134259 |
| [41] | Martin, J. W., Carballido, E. M. et. al: Squamous cell carcinoma of the urinary bladder: Systematic review of clinical characteristics and therapeutic approaches. Arab journal of urology. 14: 183-191. |
| [42] | Umair, Marvi & Rahat, Noshaba & Momin, Zumrud & Siraj, Farah & Bashir, Prih & Shezad, Humera. (2022: Histopathological Evaluation of Neoplastic and Non- neoplastic Lesions of Urinary Bladder: A Five-year Experience from a Tertiary Care Center. https://doi.org/10.31782/IJCRR.2022.14917 |
[38-42]
. In a study done in Croatia, gross hematuria was associated with detection of high-grade bladder cancer and larger tumor size
| [39] | Hamdi Y, Abdeljaoued-Tej I, Zatchi AA, Abdelhak S, Boubaker S, Brown JS, Benkahla A: Cancer in Africa: The Untold Story. Front Oncol. 2021, 15: 650117. https://doi.org/10.3389/fonc.2021.650117 |
| [43] | Nambiar AK, Arlandis S, Bø K, Cobussen-Boekhorst H, Costantini E, de Heide M, Farag F, Groen J, Karavitakis M, Lapitan MC, Manso M, Arteaga SM, Riogh ANA, O'Connor E, Omar MI, Peyronnet B, Phé V, Sakalis VI, Sihra N, Tzelves L, van Poelgeest-Pomfret ML, van den Bos TWL, van der Vaart H, Harding CK. European Association of Urology Guidelines on the Diagnosis and Management of Female Non-neurogenic Lower Urinary Tract Symptoms. Part 1: Diagnostics, Overactive Bladder, Stress Urinary Incontinence, and Mixed Urinary Incontinence. Eur Urol. 2022 Jul; 82(1): 49-59. https://doi.org/10.1016/j.eururo.2022.01.045 Epub 2022 Feb 23 |
| [44] | Barone B, Finati M, Cinelli F et. al: Bladder Cancer and Risk Factors: Data from a Multi-Institutional LongTerm Analysis on Cardiovascular Disease and Cancer Incidence. J Pers Med. 2023, 13: 512. https://doi.org/10.3390/jpm13030512 |
| [45] | Cassell A, Yunusa B et. al: Non-Muscle Invasive Bladder Cancer: A Review of the Current Trend in Africa. World J Oncol. 2019, 10: 123-131. https://doi.org/10.14740/wjon1210 |
[39, 43-45]
.
5. Limitation of This Study
1. There were incomplete clinical information and some missing request papers affecting the study.
2. Being cross-sectional study is another limitation of our study.
6. Conclusion
In this study, we explored a wide spectrum of bladder lesions, encompassing both neoplastic and non-neoplastic conditions. Among the key findings, hematuria emerged as the predominant characteristic in nearly all transurethral resection of bladder tumor (TURBT) specimens. The majority of cases were malignant neoplasms, with invasive urothelial carcinoma being the prevailing subtype. Notably, the male-to-female ratio was 4:1, and the most common age group affected was individuals in their fifth and sixth decades of life. And there was a significant association between neoplastic nature bladder lesions and sample size received and age of the patients.
The study revealed several subtype morphologies of urothelial carcinoma, which, due to their resemblance to other malignancies and benign lesions, posed diagnostic challenges. Urothelial papilloma emerged as the most prevalent benign tumor, while chronic nonspecific cystitis and cystitis cystica were the most frequent non-neoplastic lesions encountered in routine practice.
Overall, our findings align with previous research, emphasizing the increasing trend of urothelial carcinoma. The clinicopathological features, prevalence, and distribution of various bladder lesion types observed in this study mirror those documented in earlier investigations.
7. Recommendation
1. Improvements in TURBP procedures would be beneficial because muscle invasion is important in management and prognosis, yet the most of TURBT specimens lacked muscle proper, large amount of sample need to be sent as there are associations between sample size and neoplastic nature of the lesion.
2. Muscle content should be noted on biopsy samples on a regular basis.
3. Patients with muscle-invasive bladder cancer require cystectomies, but thee hospitals don't often do these procedures, therefore it's important that they do.
4. Interdepartmental relationships between pathologists and doctors might be beneficial in order to reduce the incomplete filling of some biopsy requests.
5. Some patient medical records were managed improperly and with inadequate information. As a result, the hospital's record archiving needs to be enhanced. A sustainable digital data archiving system needs to be implemented, and ongoing training and audits are required.
6. Awareness needs to be created in the adult and elderly about bladder cancer, since there is a significant association between neoplastic bladder lesions and age.
Abbreviations
BC | Bladder Cancer |
BOO | Bladder Outlet Obstruction |
GLOBOCAN | Global Cancer Incidence, Mortality, and Prevalence |
HGPUC | High Grade Papillary Urothelial Carcinoma |
LGPUC | Low Grade Papillary Urothelial Carcinoma |
LUTS | Lower Urinary Tract Symptom |
PUNLMP | Papillary Urothelial Neoplasm of Low Malignant Potential |
SCC | Squamous Cell Carcinoma |
TCC | Transitional Cell Carcinoma |
TURBT | Trans-Urethral Resection of Bladder Tumor |
WHO | World Health Organization |
Author Contributions
Ghion Getenet Engida: Conceptualization, Validation, Writing – original draft, Writing – review & editing
Abebe Melis Nisiro: Conceptualization, Investigation, Supervision, Writing – review & editing
Fanuel Belayneh Bekele: Conceptualization, Validation, Writing – review & editing
Teketel Tadesse Geremew: Conceptualization, Investigation, Methodology, Supervision, Validation, Writing – review & editing
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The raw data used in present study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Juan Rosai: Rosai and Ackerman's Surgical Pathology, tenth edition. Philadelphia: Elsevier; 2011.
|
| [2] |
Shermadou ES, Rahman S, Leslie SW: Anatomy, Abdomen and Pelvis: Bladder. [Updated 2023 Jul 24]. In StatPearls [Internet, Treasure Island (FL): StatPearls Publishing; 2023.
|
| [3] |
Mahesh Kumar U, B. R. Yelikar: Spectrum of lesions in cystoscopic bladder biopsies-A histopathological study. AJMS. 2012, 5132: 36.
https://doi.org/10.7860/JCDR/2013/5166.3233
|
| [4] |
GLOBOCAN. 2020, 10: 2020.
https://doi.org/10.3322/caac.21660
|
| [5] |
Ploeg M, Aben KK, Kiemeney LA: The present and future burden of urinary bladder cancer in the world. World J Urol. 2009, 27: 289-93.
https://doi.org/10.1007/s00345-009-0383-3
|
| [6] |
Saginala K, Barsouk A, Aluru JS, Rawla P, Padala SA, Barsouk A: Epidemiology of Bladder Cancer. Med Sci (Basel. 2020, 13: 7151633.
https://doi.org/10.3390/medsci8010015
|
| [7] |
Jozwicki W, Domaniewski J, Skok Z, et al.: Usefulness of histologic homogeneity estimation of muscleinvasive urinary bladder cancer in an individual prognosis: A mapping study. Urology. 2005, 66: 1122-6.
https://doi.org/10.1016/j.urology.2005.06.134
|
| [8] |
Domanowska E, Jozwicki W, Domaniewski J, et al.: Muscle-invasive urothelial cell carcinoma of the human bladder: Multidirectional differentiation and ability to metastasize. Hum Pathol. 2007, 38: 741-6.
https://doi.org/10.1016/j.humpath.2006.11.001
|
| [9] |
Lenis AT, Lec PM, Chamie K, Mshs MD: Bladder Cancer: A Review. JAMA. 2020, 17: 1980-1991.
https://doi.org/10.1001/jama.2020.17598
|
| [10] |
Mazzucchelli R, Marzioni D, Tossetta G, Pepi L, Montironi R: Bladder Cancer Sample Handling and Reporting: Pathologist's Point of View. Front Surg. 202128, 754741:
https://doi.org/10.10.3389/fsurg.2021.754741
|
| [11] |
Bayraktar Z, Gurbuz G, Taşci AI, Sevin G: Staging error in the bladder tumor: the correlation between stage of TUR and cystectomy. Int Urol Nephrol. 2001: 627-9.
https://doi.org/10.1023/a: 1020553812554
|
| [12] |
Chalasani V, Chin JL, Izawa JI: Histologic variants of urothelial bladder cancer and nonurothelial histology in bladder cancer. Can Urol Assoc J. 2009, 4: 193-8.
https://doi.org/10.5489/cuaj.1195
|
| [13] |
Cumberbatch MGK, Jubber I, Black PC, et al.: Epidemiology of bladder cancer: a systematic review and contemporary update of risk factors in 2018. Eur Urol. 2018, 74: 784-795.
https://doi.org/10.1016/j.eururo.2023.03.029
|
| [14] |
Wu X, Ros MM, Gu J, Kiemeney L (2008: Epidemiology and genetic susceptibility to bladder cancer. BJU Int. 102: 1207-1215.
https://doi.org/10.1111/j.1464-410X.2008.07961.x
|
| [15] |
Global cancer observatory. International Agency for Research on Cancer, WHO. Incidence, Mortality, 2020.
|
| [16] |
Adeloye D, Harhay et. al: Estimate of the incidence of bladder cancer in Africa: A systematic review and Bayesian meta-analysis. Int J Urol. 2019, 26: 102-112.
https://doi.org/10.1111/iju.13824
|
| [17] |
Genebo, Asmare, Assefa: ScienceDirect, Cancer Epidemiology, First. 53: 93-98.
https://doi.org/10.1016/j.canep.2018.01.008
|
| [18] |
Priyamvada Singhal1, Mitali Singhal2, Mamta Gupta3: Rani Bansal Histopathological Spectrum of Neoplastic and Non Neoplastic Lesions of Urinary Bladder- A Retrospective Study. 2021.
https://doi.org/10.3126/nmj.v4i2.41353
|
| [19] |
Manisha Shrestha1, Dipti Gautam1, Prakriti Shah1, Prateek Krishna Shrestha: Histopathological Spectrum of Nonneoplastic and Neoplastic Lesions of Urinary Bladder Nepalese Medical Journal, (2021) Vol. 4, 473- 477.
https://doi.org/10.7860/NJLM/2021/46894.2537
|
| [20] |
Suba G, Gayathri J, Jayaprakash HT: Histopathological overview of cystoscopic bladder biopsies- A retrospective analysis. Trop J Path Micro. 2017, 3: 229-234.
https://doi.org/10.17511/jopm.2017.i02.27
|
| [21] |
Sasikumar, S., Wijayarathna, K. S. N. et. al: A., & Abeygunasekera, A. M. Pathological Characteristics of Primary Bladder Carcinoma Treated at a Tertiary Care Hospital and Changing Demographics of Bladder Cancer in Sri Lanka. Advances in Urology. 201616,
https://doi.org/10.1155/2016/5751647
|
| [22] |
C. Aparna, M. D, Rayapa Reddy Thumma, C Padmavathi Devi, S V R L Jyothi Vanapalli, T D N Mounika: histological Spectrum of Urothelial Lesions - Experience of A Single Tertiary. Care Institute, international Journal of Contemporary Medical Research Volume 3 | Issue 6 | June. 2016.
|
| [23] |
Anita Shah, Manglesh Srivastava, Ashok Samdurkar, Ghanshyam Sigdel SPECTRUM OF LESIONS IN URINARY BLADDER: A HISTOPATHOLOGICAL STUDY Journal of Universal College of Medical Sciences. 6: 24-27.
https://doi.org/10.3126/jucms.v6i2.22473
|
| [24] |
A CLINICO-HISTOPATHOLOGICAL STUDY OF URINARY BLADDER LESIONS Siddhi Kumari Pandey1, Ranu Tiwari Mishra2, F: S. Solanki3, Sanjay Totade4, Jagmohan Singh Dhakar5International Journal of Academic Medicine and Pharmacy. ISSN (O):: 2687-5365.
|
| [25] |
El-Siddig AA, Albasri AM, Hussainy AS, Alhujaily AS: Urinary bladder cancer in adults: a histopathological experience from Madinah, Saudi Arabia. J Pak Med Assoc. 2017, 67: 83-86.
|
| [26] |
Forae, GeraldDafe & Ugiagbe, EzekielEnoghama & Mekoma, DikeFidelis. (2016: A descriptive study of bladder tumors in Benin City, Nigeria: An analysis of histopathological patterns. Saudi surgical journal. 4: 113.
https://doi.org/10.4103/2320-3846.193986
|
| [27] |
Muhammed Mubarak, Javed I. Kazi, Altaf Hashmi, Manzoor Hussain, Syed Anwer Naqvi, Syed Adeebul Hassan Rizvi: Urinary Bladder Tumors in Southern. Pakistan: A Histopathological Perspective, Middle East Journal of Cancer; July. 2014, 5: 167-173.
|
| [28] |
Ferlay J: Global cancer observatory: cancer today.
https://gco.iarc.fr/today.10.1002/ijc.31937
|
| [29] |
H Biluts, E Minas: Bladder Tumors at Tikur Anbessa Hospital in Ethiopia. East and Central African Journal of Surgery, Volume. 16: 1.
https://doi.org/10.4103/aam.aam_48_17
|
| [30] |
Billis A, Schenka AA, Ramos CC, Carneiro LT, Araújo V: Squamous and/or glandular differentiation in urothelial carcinoma: prevalence and significance in transurethral resections of the bladder. Int Urol Nephrol. 2001: 631-3.
https://doi.org/10.1023/a: 1020597611645
|
| [31] |
Wasco MJ, Daignault S, Zhang Y, Kunju LP et. al: Urothelial carcinoma with divergent histologic differentiation (mixed histologic features) predicts the presence of locally advanced bladder cancer when detected at transurethral resection. Urology. 2007, 70: 69-74.
https://doi.org/10.1016/j.urology.2007.03.033
|
| [32] |
Shah RB, Montgomery JS, Montie JE, Kunju LP: Variant (divergent) histologic differentiation in urothelial carcinoma is under-recognized in community practice: impact of mandatory central pathology review at a large referral hospital. Urol Oncol. 2013, 31: 1650-5.
https://doi.org/10.1016/j.urolonc.2012.04.009
|
| [33] |
Boustead GB, Fowler S, Swamy R, Kocklebergh R, Hounsome L: Section of Oncology, BAUS. Stage, grade and pathological characteristics of bladder cancer in the UK: British Association of Urological Surgeons (BAUS) urological tumour registry. BJU Int. 2014, 113: 924-30.
https://doi.org/10.1111/bju.12468
|
| [34] |
Amin HAA, Kobaisi MH, Samir RM: Schistosomiasis and Bladder Cancer in Egypt: Truths and Myths. Open Access Maced J Med Sci. 2019, 10: 4023-4029.
https://doi.org/10.3889/oamjms.2019.857
|
| [35] |
Chamie K, Ballon-Landa E, Bassett JC, Daskivich TJ, Leventhal M, Deapen D, Litwin MS: Quality of diagnostic staging in patients with bladder cancer: a process-outcomes link. Cancer. 2015, 1: 379-85
https://doi.org/10.1002/cncr.29071
|
| [36] |
Hodges KB, Lopez-Beltran A, Maclennan GT, Montironi R, Cheng L: Urothelial lesions with inverted growth patterns: histogenesis, molecular genetic findings, differential diagnosis and clinical management. BJU Int. 2011, 107: 532-7.
https://doi.org/10.1111/j.1464-410X.2010.09853.x
|
| [37] |
Dive AM, Bodhade AS, Mishra MS, Upadhyaya N: Histological patterns of head and neck tumors: An insight to tumor histology. J Oral Maxillofac Pathol. 2014, 18: 58-68.
https://doi.org/10.4103/0973-029X.131912
|
| [38] |
Cao M, Yang G, Pan et. al: Repeated transurethral resection for non-muscle invasive bladder cancer. Int J Clin Exp Med. 2015, 15: 1416-9.
|
| [39] |
Hamdi Y, Abdeljaoued-Tej I, Zatchi AA, Abdelhak S, Boubaker S, Brown JS, Benkahla A: Cancer in Africa: The Untold Story. Front Oncol. 2021, 15: 650117.
https://doi.org/10.3389/fonc.2021.650117
|
| [40] |
Dora, Jakus., Ivan, Šolić., J. et. al: The Impact of the Initial Clinical Presentation of Bladder Cancer on Histopathological and Morphological Tumor Characteristics. 12: 4259-4259.
https://doi.org/10.3390/jcm12134259
|
| [41] |
Martin, J. W., Carballido, E. M. et. al: Squamous cell carcinoma of the urinary bladder: Systematic review of clinical characteristics and therapeutic approaches. Arab journal of urology. 14: 183-191.
|
| [42] |
Umair, Marvi & Rahat, Noshaba & Momin, Zumrud & Siraj, Farah & Bashir, Prih & Shezad, Humera. (2022: Histopathological Evaluation of Neoplastic and Non- neoplastic Lesions of Urinary Bladder: A Five-year Experience from a Tertiary Care Center.
https://doi.org/10.31782/IJCRR.2022.14917
|
| [43] |
Nambiar AK, Arlandis S, Bø K, Cobussen-Boekhorst H, Costantini E, de Heide M, Farag F, Groen J, Karavitakis M, Lapitan MC, Manso M, Arteaga SM, Riogh ANA, O'Connor E, Omar MI, Peyronnet B, Phé V, Sakalis VI, Sihra N, Tzelves L, van Poelgeest-Pomfret ML, van den Bos TWL, van der Vaart H, Harding CK. European Association of Urology Guidelines on the Diagnosis and Management of Female Non-neurogenic Lower Urinary Tract Symptoms. Part 1: Diagnostics, Overactive Bladder, Stress Urinary Incontinence, and Mixed Urinary Incontinence. Eur Urol. 2022 Jul; 82(1): 49-59.
https://doi.org/10.1016/j.eururo.2022.01.045
Epub 2022 Feb 23
|
| [44] |
Barone B, Finati M, Cinelli F et. al: Bladder Cancer and Risk Factors: Data from a Multi-Institutional LongTerm Analysis on Cardiovascular Disease and Cancer Incidence. J Pers Med. 2023, 13: 512.
https://doi.org/10.3390/jpm13030512
|
| [45] |
Cassell A, Yunusa B et. al: Non-Muscle Invasive Bladder Cancer: A Review of the Current Trend in Africa. World J Oncol. 2019, 10: 123-131.
https://doi.org/10.14740/wjon1210
|
Cite This Article
-
APA Style
Engida, G. G., Nisiro, A. M., Bekele, F. B., Geremew, T. T. (2024). Histopathologic Patterns of Urinary Bladder Lesions and Associated Factors in Hawassa University Comprehensive Specialized Hospital, Sidama Region, Ethiopia. International Journal of Clinical Urology, 8(2), 23-34. https://doi.org/10.11648/j.ijcu.20240802.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Engida, G. G.; Nisiro, A. M.; Bekele, F. B.; Geremew, T. T. Histopathologic Patterns of Urinary Bladder Lesions and Associated Factors in Hawassa University Comprehensive Specialized Hospital, Sidama Region, Ethiopia. Int. J. Clin. Urol. 2024, 8(2), 23-34. doi: 10.11648/j.ijcu.20240802.13
Copy
|
Download
AMA Style
Engida GG, Nisiro AM, Bekele FB, Geremew TT. Histopathologic Patterns of Urinary Bladder Lesions and Associated Factors in Hawassa University Comprehensive Specialized Hospital, Sidama Region, Ethiopia. Int J Clin Urol. 2024;8(2):23-34. doi: 10.11648/j.ijcu.20240802.13
Copy
|
Download
-
@article{10.11648/j.ijcu.20240802.13,
author = {Ghion Getenet Engida and Abebe Melis Nisiro and Fanuel Belayneh Bekele and Teketel Tadesse Geremew},
title = {Histopathologic Patterns of Urinary Bladder Lesions and Associated Factors in Hawassa University Comprehensive Specialized Hospital, Sidama Region, Ethiopia
},
journal = {International Journal of Clinical Urology},
volume = {8},
number = {2},
pages = {23-34},
doi = {10.11648/j.ijcu.20240802.13},
url = {https://doi.org/10.11648/j.ijcu.20240802.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20240802.13},
abstract = {Background: Urinary bladder lesions, non-neoplastic and neoplastic, are collectively responsible for significant morbidity and mortality throughout the world. Bladder cancer is a prevalent disease affects a significant number of individuals each year worldwide. The most common non-neoplastic and neoplastic lesion of the urinary bladder is non-specific cystitis and urothelial carcinoma respectively. Objectives: The aim of this study is to describe histopathologic patterns of urinary bladder lesions and associated risk factors in Hawassa University Comprehensive Specialized Hospital from January 2017 to December 2023. Methods: A 7-year cross sectional study was conducted to describe histologically diagnosed bladder lesions and associated factors at Hawassa University Comprehensive Specialized Hospital from January 2017 to December 2023. Results: This study comprised a total of 182 patients who have bladder biopsies at Hawassa University Comprehensive Specialized Hospital, Pathology department from January 2017 to December 2023. Out of which 21 cases (12.1%) are non-neoplastic, while 152 cases (83%) are neoplastic. Nine cases (4.9%) have a descriptive diagnosis. With 139 (90.44%) cases, urothelial neoplasms have the highest frequency form all neoplastic lesions. Ninety-seven cases, or 69.8%, of urothelial neoplasms were invasive; of them, 78 (80.4%) were high grade cases. Low-grade noninvasive papillary carcinomas, which accounted for 24 instances. One case is a cystectomy specimen, and the remaining 181 cases are TURBT. The age range of 50-59 years was the most frequent accounting for 39 (21.4%) of all cases, with a male to female (M: F) ratio of 2.9:1. The most frequent presenting symptom in 146 (85.7%) of patients was hematuria. Conclusions: This study demonstrates that 139 (90.44%) of the neoplastic bladder lesions were bladder neoplasms of urothelial origin, 97 (69.8%) of which are invasive urothelial carcinoma with rising numbers each year and implying the burden in the region.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - Histopathologic Patterns of Urinary Bladder Lesions and Associated Factors in Hawassa University Comprehensive Specialized Hospital, Sidama Region, Ethiopia
AU - Ghion Getenet Engida
AU - Abebe Melis Nisiro
AU - Fanuel Belayneh Bekele
AU - Teketel Tadesse Geremew
Y1 - 2024/10/18
PY - 2024
N1 - https://doi.org/10.11648/j.ijcu.20240802.13
DO - 10.11648/j.ijcu.20240802.13
T2 - International Journal of Clinical Urology
JF - International Journal of Clinical Urology
JO - International Journal of Clinical Urology
SP - 23
EP - 34
PB - Science Publishing Group
SN - 2640-1355
UR - https://doi.org/10.11648/j.ijcu.20240802.13
AB - Background: Urinary bladder lesions, non-neoplastic and neoplastic, are collectively responsible for significant morbidity and mortality throughout the world. Bladder cancer is a prevalent disease affects a significant number of individuals each year worldwide. The most common non-neoplastic and neoplastic lesion of the urinary bladder is non-specific cystitis and urothelial carcinoma respectively. Objectives: The aim of this study is to describe histopathologic patterns of urinary bladder lesions and associated risk factors in Hawassa University Comprehensive Specialized Hospital from January 2017 to December 2023. Methods: A 7-year cross sectional study was conducted to describe histologically diagnosed bladder lesions and associated factors at Hawassa University Comprehensive Specialized Hospital from January 2017 to December 2023. Results: This study comprised a total of 182 patients who have bladder biopsies at Hawassa University Comprehensive Specialized Hospital, Pathology department from January 2017 to December 2023. Out of which 21 cases (12.1%) are non-neoplastic, while 152 cases (83%) are neoplastic. Nine cases (4.9%) have a descriptive diagnosis. With 139 (90.44%) cases, urothelial neoplasms have the highest frequency form all neoplastic lesions. Ninety-seven cases, or 69.8%, of urothelial neoplasms were invasive; of them, 78 (80.4%) were high grade cases. Low-grade noninvasive papillary carcinomas, which accounted for 24 instances. One case is a cystectomy specimen, and the remaining 181 cases are TURBT. The age range of 50-59 years was the most frequent accounting for 39 (21.4%) of all cases, with a male to female (M: F) ratio of 2.9:1. The most frequent presenting symptom in 146 (85.7%) of patients was hematuria. Conclusions: This study demonstrates that 139 (90.44%) of the neoplastic bladder lesions were bladder neoplasms of urothelial origin, 97 (69.8%) of which are invasive urothelial carcinoma with rising numbers each year and implying the burden in the region.
VL - 8
IS - 2
ER -
Copy
|
Download